If you are a patient with age-related macular degeneration (AMD), or you know someone who is affected, you may have wondered if daily supplements really help. Can a vitamin formula slow the progression of vision loss caused by AMD? The National Eye Institute (NEI) says Yes. Upon completion of a 10-year follow-on study, the NEI reaffirms its recommendation of the nutrient formula, known as AREDS2, confirming it continues to deliver positive results in slowing the progression of vision loss in patients with intermediate to advanced AMD. Macular degeneration is a leading cause of central vision loss in people over age 50. As the disease progresses it can seriously impair a person’s ability to read, recognize faces or drive.
The NEI has been looking at the effects of supplemental nutrients on AMD for 20 years now. The specific mix of vitamins, minerals and antioxidants originated in the 2001 Age-Related Eye Disease Study (AREDS) which focused on a combination of antioxidants and zinc. In the second study, AREDS2, which was completed in 2012, the NEI tested changes to the formulation, including the addition of omega-3 fatty acids, substituting lutein and zeaxanthin for beta-carotene, and reducing zinc. The formulation included in the 2012 study is the AREDS2 formula this long-term study was based on.
The formulation is the same combination found in PreserVision AREDS2 eye vitamins by Bausch & Lomb. which was provided to participants during the last 5-years of this study. The daily dose contains the recommended levels of all six clinically proven nutrients: vitamin C (500mg), vitamin E (400 IU/180mg), lutein (10mg), zeaxanthin (2mg), zinc (80mg zinc oxide), and copper (2mg cupric oxide). The AMD nutrient formula can also be found in other brands including: I-Caps AREDS 2 (Alcon), Eyepex Macula (Eyepex Formulas) or MacularProtect Complete AREDS2.
The AREDS2 vitamins are formulated exclusively for AMD patients with intermediate to advanced disease. Consult your doctor before taking these supplements. Keep in mind, vitamin supplements are not a replacement for good nutrition, your diet should be rich in all these nutrients to derive best results. Read about the incomparable benefits of a healthy fresh Mediterranean diet in The Anti-AMD Diet. And remember it’s also important to maintain a healthy weight, protect your eyes from the sun and do not smoke!
Vaccinations are a significant step in moving forward from the COVID-19 pandemic.Although it is what we’ve been waiting for, the reopening of business and social activities, to full capacity, may not feel comfortable for a while. It’s okay to exercise your options and take smaller incremental steps, instead of throwing all caution to the wind.
Adjusting and getting back a sense of normal are experiences people with vision loss know all too well, but that does not make this process any easier. It should remind us, however, that change always takes time and often leaves us temporarily feeling weird and awkward. Managing reentry, into social gatherings and public spaces may not be as glee-filled for everyone.So go ahead, proceed at your own pace, do it your way.
The rules and regulations of the 2020 pandemic were largely thrust upon us. Re-entry offers an opportunity to write the next chapter, individually recovering from this massive disruption, stronger, smarter, and happier.
Be kind to yourself.
Take it easy, now is the time to consciously reduce the stress load our brains have been carrying.It’s okay to be selective and keep commitments light. Prioritize your mental health and physical well-being on a daily basis. Develop better nutrition and sleep habits. Showing yourself patience and grace strengthens your reserve for compassion to others.
Two Image shows two vaccinated women enjoying coffee together, post-pandemic restrictions.
Ease back in with small incremental steps.
Begin by celebrating reentry with one close friend (or two, vaccinated of course)in a social setting, then move on to more. Keep it small and outdoors, if that’s what makes you feel happy and secure. It may take some time to work up to larger gatherings.Negotiate a phased-in return to the office and keep the conferences virtual for a time. Ease back into public transportation with a travel schedule that accommodates your comfort.And take another look at OE’s 2021 theme article: This Year Small Changes are Big.
Take time to appreciate.
The simple act of recognizing and expressing thankfulness, each day, promotes happiness. Research shows the practice of gratitude fortifies our resolve, builds resilience, and improves overall mental health. Whether you write it, think it or share it, the more you do the better you get.
Removing the mask.
As this article is written, the CDC announces, it is safe for fully vaccinated people to stop wearing masks and they no longer need to maintain social distance, indoors or out. Masks will continue to be required when visiting medical offices, hospitals or long-term care facilities. The mask, unwelcome by some, provided others a real sense of safety. It won’t be easy for everyone to drop it overnight. Feel free to mask at your discretion, it is, after all, a sign of respect for the health of others.
The next phase is your chapter to write. Think about reevaluating. Things are changing anyway, so take the time to consider which routines, behaviors and activities you want to improve. Think small — not epic.
Once upon a time, not so long ago, people believed that age-related macular degeneration caused total blindness. Today we know better. AMD affects people over age 50, resulting in a blurring of the sharp central vision used for reading, driving, identifying faces, and other detail oriented tasks. The peripheral vision is not affected and can be helpful in compensating. The dry form of AMD accounts for about 90% of cases, marked by slowly progressing changes. The remaining 10% have the wet form which causes more aggressive vision loss due to leaking blood vessels behind the eye. Treatment is available and effective in managing wet AMD.Patients are able to continue a productive and independent life with the active implementation of small changes and the embrace of technology.
Here is a collection of OE’s recent and most popular content on the subject, in recognition of AMD Awareness Month – February 2021.
Closeup of elderly woman’s eye
What Is AMD?
An explanation of age-related macular degeneration, thorough and well presented for review as an informative introduction or to refresh your knowledge. Read Now
Image of the logo for The Retina Counselor.
Emerging Treatments For AMD
A primer on clinical trials in the process for the next generation treatment and management of wet and dry age-related macular degeneration with an emphasis on more efficient and convenient patient care. Read Now
OE Patients Podcast in white text with magenta and white OE Patients logo.
Episode 14: The Retina Counselor
Listen in as Dr. Mrinali Gupta discusses the future of AMD treatments and how patients can best utilize the Retina Counselor report. Listen Now
Fresh vegetables and fruits spread out on a gray table.
The Anti-AMD Diet
This is one of OE Patients most popular articles. Improving nutrition habits through small dietary changes has been found to prevent and slow the development of AMD. Read Now
Older woman using digital tablet outdoors
Living Better With AMD
Patients should be to be well informed that although there may be no medical treatments available yet, for their AMD, it most certainly does not mean “nothing can be done.” Read this article for five ways to take action. Read Now
Dahlov Ipcar “Sunlight in Forest Glade” (unfinished, 2015)
Artists Work Through Macular Degeneration
If you think AMD is a career-ending diagnosis for a visual artist, this article will change your thinking. These artists continued to thrive, despite vision loss, and you can too! Read Now
Three generations of a family sitting on a park bench.
Hope For Age-Related Macular Degeneration
Progress with age-related macular degeneration shows a promising hope for the future. Read Here for what you need to know and what you can expect. Read Now
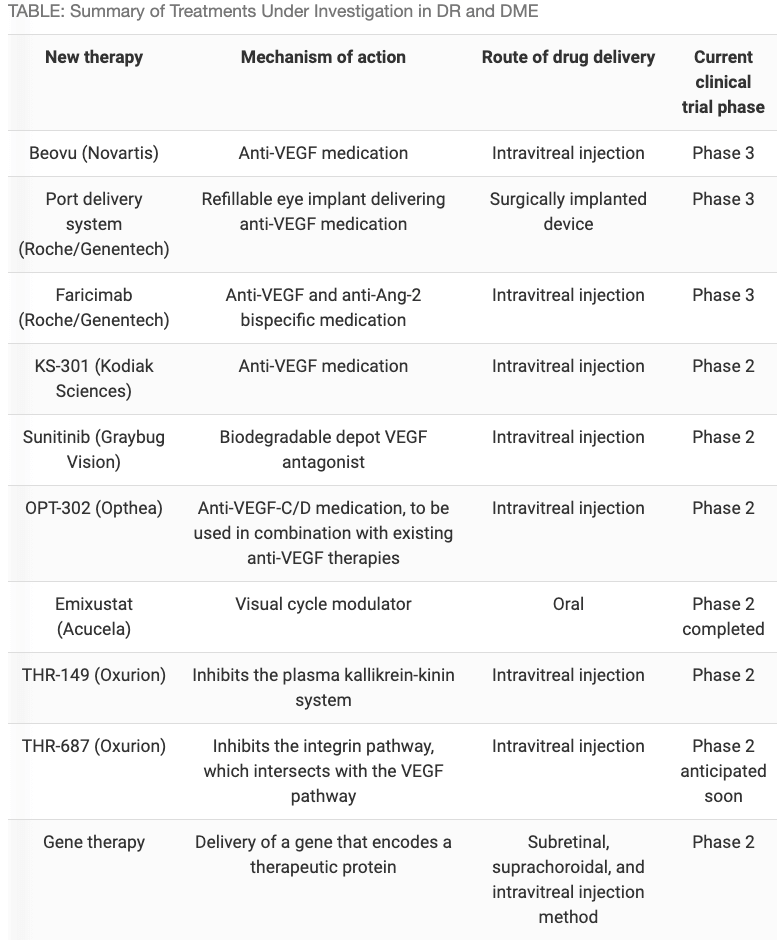
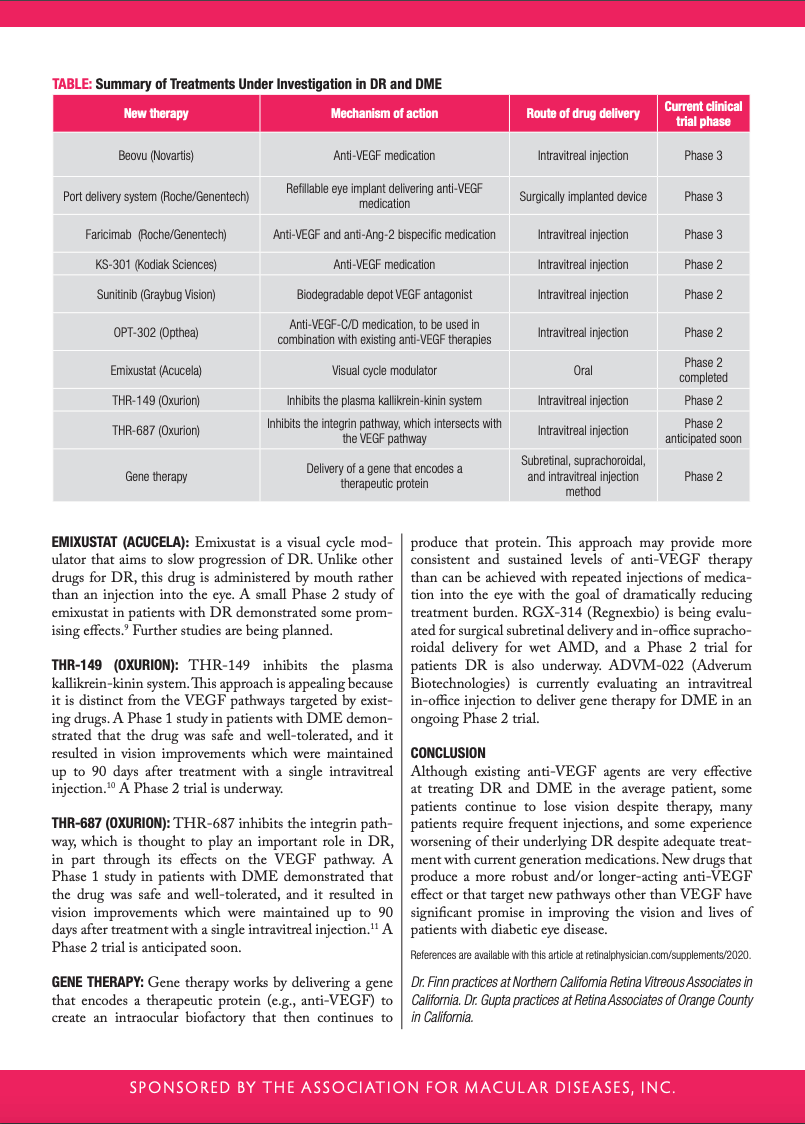
Current drug treatments for both diabetic retinopathy (DR) and diabetic macular edema (DME) are aimed at inhibiting a molecule called vascular endothelial growth factor (VEGF) or employ steroids to broadly treat inflammatory mediators present in DME and DR. The anti-VEGF medications currently include Avastin, Lucentis and Eylea, while the steroid-based treatments include triamcinolone acetonide, Ozurdex, and Illuvien. Many patients need frequent injections of these drugs, and some experience worsening of their vision or their DR despite treatment with these agents. Given these limitations, clinical trials are underway to evaluate new therapies that could provide therapeutic effect for a longer duration and/or target other pathways. Here we summarize several such therapies under investigation, primarily focusing on late-stage clinical trials (Phases 2 & 3).
BEOVU (NOVARTIS): Beovu (brolocizumab) is an antibody fragment inhibiting VEGF. The medication’s smaller size and higher molar concentration enable it to have a strong effect in treating fluid and potentially longer duration of action. Data from a Phase 3 trial evaluating the medication for wet age-related macular degeneration (AMD) showed more than half of patients were able to continue on a 3-month dosing regimen with Beovu through 1 year.1 However, there are safety concerns with this medication due to intraocular inflammation and occlusive retinal vasculitis occurring in some patients receiving the medication for AMD.2
PORT DELIVERY SYSTEM (GENENTECH): This treatment consists of a small refillable device that stores and continuously releases anti-VEGF medication into the eye by diffusion, taking the place of frequent injections. The device is surgically implanted into the wall of the eye. The tiny implant can then be refilled in the office with medication as needed. Current studies evaluating patients with wet AMD showed the majority of patients could go 6 months before needing retreatment.3 Enrollment for Phase 3 clinical trials evaluating this device for use in patients with DME and DR are ongoing.
FARICIMAB (GENENTECH): Faricimab inhibits two pathways leading to abnormal blood vessel growth and leakage: It binds and inactivates a molecule called angiopoietin-2 (Ang-2) in addition to the VEGF molecule that current medications inhibit. The goal of this dual inhibition is to potentially improve outcomes and durability of the treatment. A Phase 2 trial comparing faricimab with Lucentis showed improved visual acuity gains with faricimab as well as improvements in the severity of DR. Also, this study showed that many patients receiving faricimab could go up to 12 or even 16 weeks before needing retreatment, decreasing frequent treatment burden for these patients.4 Two Phase 3 clinical trials evaluating faricimab for DME are currently underway.
KSI-301 (KODIAK SCIENCES): KSI-301 is a specially formulated anti-VEGF drug called an antibody polymer conjugate. The medication is expected to stick around the eye for a longer time and deliver a greater dose of medication with one injection. Early-stage studies of the medication showed that over 70% of patients with DME were able to go more than 4 months without needing retreatment after an initial three loading doses.5 Larger trials evaluating the drug for use in DME and DR are currently underway.
SUNITINIB (GRAYBUG VISION): Sunitinib is a specially formulated depot medication that slowly dissolves over time in the eye. This medication is a tyrosine kinase inhibitor that blocks VEGF receptors. After the medication is injected, its small particles aggregate or stick together and slowly release over time, allowing for the possibility of an extended treatment effect.6 Early stage trials showed the medication could last up to 6 months in the majority of patients with wet AMD.7The medication is currently in a Phase 2 trial for patients with DME.
OPT-302 (OPTHEA): OPT-302 inhibits VEGF-C and VEGF-D and is designed to be used in combination with the existing therapies, which target VEGF-A or VEGF-A and B. The rationale is that blocking additional VEGF family members will yield a more potent and longer-lasting anti-VEGF effect. Preliminary data from an ongoing Phase 2a trial suggests that combination therapy with Eylea and intravitreal OPT-302 yields superior vision outcomes than treatment with Eylea alone in eyes with DME.8 Phase 3 trials may be performed in the future.
EMIXUSTAT (ACUCELA): Emixustat is a visual cycle modulator that aims to slow progression of DR. Unlike other drugs for DR, this drug is administered by mouth rather than an injection into the eye. A small Phase 2 study of emixustat in patients with DR demonstrated some promising effects.9 Further studies are being planned.
THR-149 (OXURION): THR-149 inhibits the plasma kallikrein-kinin system. This approach is appealing because it is distinct from the VEGF pathways targeted by existing drugs. A Phase 1 study in patients with DME demonstrated that the drug was safe and well-tolerated, and it resulted in vision improvements which were maintained up to 90 days after treatment with a single intravitreal injection.10 A Phase 2 trial is underway.
THR-687 (OXURION): THR-687 inhibits the integrin pathway, which is thought to play an important role in DR, in part through its effects on the VEGF pathway. A Phase 1 study in patients with DME demonstrated that the drug was safe and well-tolerated, and it resulted in vision improvements which were maintained up to 90 days after treatment with a single intravitreal injection.11 A Phase 2 trial is anticipated soon.
GENE THERAPY: Gene therapy works by delivering a gene that encodes a therapeutic protein (e.g., anti-VEGF) to create an intraocular biofactory that then continues to produce that protein. This approach may provide more consistent and sustained levels of anti-VEGF therapy than can be achieved with repeated injections of medication into the eye with the goal of dramatically reducing treatment burden. RGX-314 (Regnexbio) is being evaluated for surgical subretinal delivery and in-office suprachoroidal delivery for wet AMD, and a Phase 2 trial for patients DR is also underway. ADVM-022 (Adverum Biotechnologies) is currently evaluating an intravitreal in-office injection to deliver gene therapy for DME in an ongoing Phase 2 trial.
CONCLUSION
Although existing anti-VEGF agents are very effective at treating DR and DME in the average patient, some patients continue to lose vision despite therapy, many patients require frequent injections, and some experience worsening of their underlying DR despite adequate treatment with current generation medications. New drugs that produce a more robust and/or longer-acting anti-VEGF effect or that target new pathways other than VEGF have significant promise in improving the vision and lives of patients with diabetic eye disease.
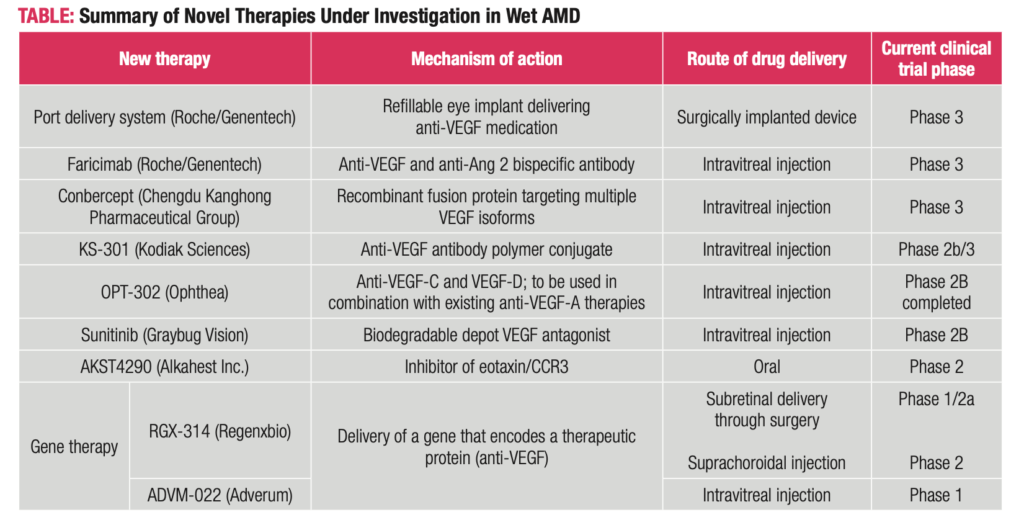
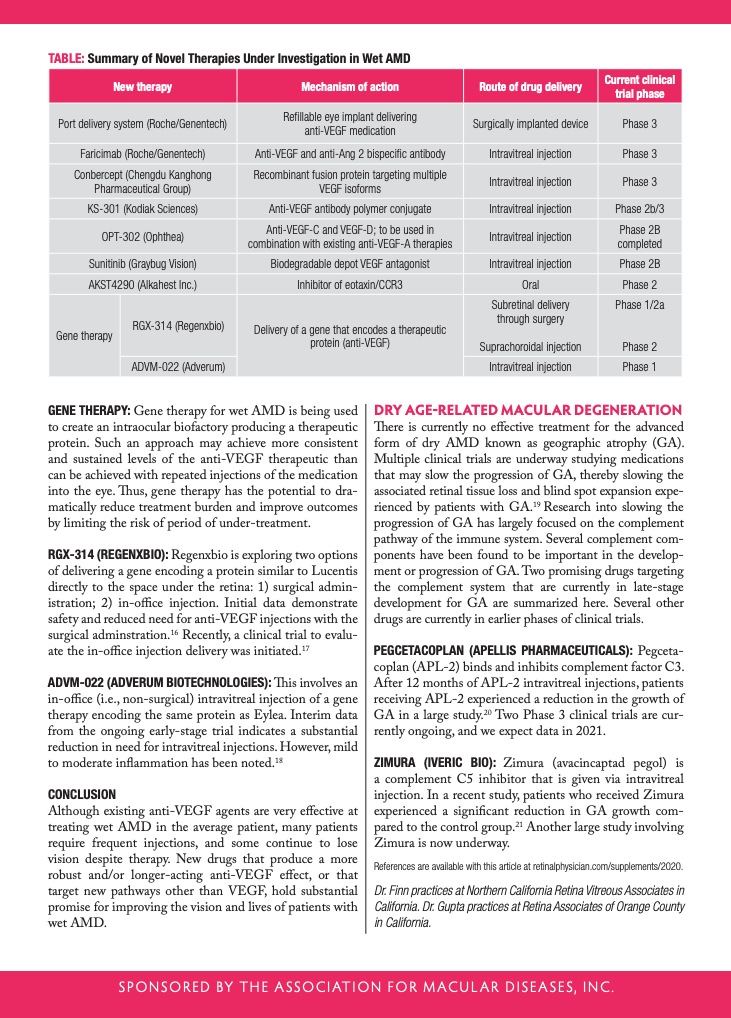
The current treatments for wet age-related macular degeneration (wAMD) inhibit a molecule called vascular endothelial growth factor (VEGF). This molecule leads to abnormal blood vessel growth and instability. Currently available anti-VEGF drugs—Avastin (Genentech),Eylea, (Regeneron), Lucentis (Genentech)—are remarkably safe and very effective for wAMD. However, with current treatments, most patients need frequent injections indefinitely. More recently, a new anti-VEGF agent, Beovu (Novartis), was FDA-approved for wAMD with suggestion of longer duration of action and reduced need for injections; however, safety concerns related to inflammation have limited widespread use of this agent. Fortunately, several clinical trials are underway to evaluate new therapies that target other pathways and/or are formulated to produce a more longer-lasting effect and, in turn, reduce treatment burden. Here, we summarize several such therapies under investigation, primarily focusing on late-stage trials (Phases 2 & 3).
Port Delivery System (Genentech):This treatment consists of a small refillable device that is implanted into the wall of the eye during a surgical procedure. The small implant stores and continuously releases anti-VEGF medication into the eye by diffusion, taking the place of frequent injections. The device can be refilled in the office. Current studies have evaluated refills every 6 months, and some early studies showed that patients could go on average about 15 months without needing a refill.1 The Port Delivery System has completed a Phase 3 clinical trial and we expect the data will be filed with the FDA soon.2
Faricimab (Genentech):Faricimab inhibits two pathways leading to abnormal blood vessel growth and leakage: It binds and inactivates a molecule called angiopoietin-2 (Ang-2) in addition to the VEGF molecule that current medications inhibit.3 By binding both molecules, faricimab may lead to improved outcomes and longer treatment duration.4 In current trials, the medication is being given up to every 4 months after a series of monthly doses. Phase 3 trials are ongoing, and we expect data in 2021.
Conbercept (Chengdu Kanghong):Conbercept is an engineered anti-VEGF that has been widely used in China since its approval there in 2013. It has been reported that conbercept may be a more potent medication because of its ability to address multiple targets, potentially resulting in a longer-lasting treatment (~3 months). Phase 3 trials in the U.S. are ongoing.5-6
KSI-301 (Kodiak Sciences):KSI-301 is a specially formulated anti-VEGF drug called an antibody polymer conjugate. The medication is expected to stick around the eye for a longer time and deliver a greater dose of medication with one injection.7 Patients in the ongoing trials are receiving treatment with the medication every 3 to 5 months, and some have gone up to 6 months before needing retreatment with an injection.8 A larger trial comparing KSI-301 to currently available medications is ongoing, and we expect to get data in 2021.
OPT-302 (Opthea):OPT-302 inhibits VEGF-C and VEGF-D, and is designed to be used in combination with the existing anti-VEGF-A therapies. The rationale is that blocking additional VEGF family members will yield a more potent anti-VEGF effect. A Phase 2 trial found that OPT-302 in combination with Lucentis was more effective than monthly Lucentis.9-10 Phase 3 trials are expected to start soon.
Sunitinib (Graybug):Sunitinib is a specially formulated depot medication that slowly dissolves over time in the eye.11 The medication acts in a slightly different way to inhibit VEGF.Because it is a depot, the medication releases over time, allowing for the possibility of extended treatment effect. In recent trials, 90% of patients were able to go 3 months without needing re-treatment, and 70% of patients were able to go to 6 months without needing retreatment. The medication is currently in a Phase 2 clinical trial.12
AKST4290 (Alkahest): AKST4290 is a small molecule inhibiting the immunomodulators playing a role in inflammation and neovascularization; two processes important in wAMD. This medication is unique from the others in that it is administered by mouth. Two small trials showed initial benefit of AKST4290 therapy in terms of vision stabilization and improvement.13-14 A larger
Phase 2 trial evaluating this medication is underway.15
Table: A Summary of Novel Therapies Under Investigation in Wet AMD
Gene Therapy: Gene therapy for wet AMD is being used to create an intraocular biofactory producing a therapeutic protein. Such an approach may achieve more consistent and sustained levels of the anti-VEGF therapeutic than can be achieved with repeated injections of the medication into the eye. Thus, gene therapy has the potential to dramatically reduce treatment burden and improve outcomes by limiting the risk of period of under-treatment.
RGX-314 (RegenxBio): Regenxbio is exploring two options of delivering a gene encoding a protein similar to Lucentis directly to the space under the retina: 1) surgical administration; 2) in-office injection. Initial data demonstrate safety and reduced need for anti-VEGF injections with the surgical adminstration.16 Recently, a clinical trial to evaluate the in-office injection delivery was initiated.17
ADVM-022 (Adverum Biotechnologies): This involves an in-office (i.e., non-surgical) intravitreal injection of a gene therapy encoding the same protein as Eylea. Interim data from the ongoing early-stage trial indicates a substantial reduction in need for intravitreal injections. However, mild to moderate inflammation has been noted.18
CONCLUSION
Although existing anti-VEGF agents are very effective at treating wet AMD in the average patient, many patients require frequent injections, and some continue to lose vision despite therapy. New drugs that produce a more robust and/or longer-acting anti-VEGF effect, or that target new pathways other than VEGF, hold substantial promise for improving the vision and lives of patients with wet AMD.
Dry Age-Related Macular Degeneration
There is currently no effective treatment for the advanced form of dry AMD known as geographic atrophy (GA). Multiple clinical trials are underway studying medications that may slow the progression of GA, thereby slowing the associated retinal tissue loss and blind spot expansion experienced by patients with GA.19 Research into slowing the progression of GA has largely focused on the complement pathway of the immune system. Several complement components have been found to be important in the development or progression of GA. Two promising drugs targeting the complement system that are currently in late-stage development for GA are summarized here. Several other drugs are currently in earlier phases of clinical trials.
Pegcetacoplan (Apellis Pharmaceuticals): Pegceta-coplan (APL-2) binds and inhibits complement factor C3. After 12 months of APL-2 intravitreal injections, patients receiving APL-2 experienced a reduction in the growth of GA in a large study.20 Two Phase 3 clinical trials are currently ongoing, and we expect data in 2021.
Zimura (Iveric Bio):Zimura (avacincaptad pegol) is a complement C5 inhibitor that is given via intravitreal injection. In a recent study, patients who received Zimura experienced a significant reduction in GA growth compared to the control group.21 Another large study involving Zimura is now underway.
Clinical trials are research studies that test treatments in development. They are conducted to evaluate the safety and effectiveness of medications, procedures and diagnostic methods.Studies are approved by an institutional review board to ensure the science is sound and patients are protected.
While it is a great act of generosity, volunteering to participate in a clinical trial is a serious decision which should be made with a complete understanding of the commitment involved. Although there is no guarantee you will benefit directly from the research, it’s important to understand that you are contributing to the knowledge base which is likely to help many people collectively over the long term.Discuss the clinical trial with your physician, other health care providers who are involved in your care and your family during the decision-making process.It is important that you ask any questions you might have before you make your decision.
Establishing your eligibility for a vision research study may require the diagnosis of an eye condition. Generally, subjects are screened with a medical history, physical examination, sometimes with a blood test and a comprehensive eye exam including reading a vision chart, measurement of the eye pressure and dilation to evaluate the lens, vitreous and retina. Additional screening may involve questionnaires, lab tests and non-invasive imaging.
Generally, if you participate in a clinical trial, you can receive at least some of the testing procedures for free, including the new medications/surgical procedures being evaluated. You might either receive the treatment under investigation or the standard of care for your condition. The duration of the trial and frequency of visits is variable depending on the trial and knowing this is important before you commit to participating.
Participants of clinical trials are integral to the development of treatments along with the manufacturing companies, physicians and study staff so it is important that you make this decision carefully.It is best to ask your physician or clinic staff if there are any clinical trials you would be eligible for.
Couple meet with physician to discuss participation in clinical trial.
Examples of Questions to Ask
Take time to carefully consider the criteria and the commitment. Here are the questions you should have answers for.
What is the trial’s purpose and who is the sponsor?
What are the participation criteria?
Who has reviewed and approved this study?
Has the treatment been used in other trials?
What is the investigational treatment being compared to?
How often is the treatment given?
How often will you have to come to the doctor’s office?
How long is the trial?
What are the potential benefits, short and long term?
What are the possible risks and side effects, including irreversible vision loss?
Will you incur any costs and/or will your health insurance be billed for any study procedures?
Will there by any stipend and/or coverage of transportation costs?
Informed Consent
Eligible participants must sign an Informed Consent which describes the purpose of the trial, criteria for eligibility, the treatment, potential risks and benefits, the patients’ rights and responsibilities.
Optimism and positivity are inherited traits. Studies show they can also be learned behaviors. It is never too soon, or too late, to build the skills that help us bounce back from adversity.
Facing vision loss is a daunting proposition by any standard. Although we may feel discouraged and overwhelmed at times, getting trapped in negativity is detrimental to overall health and well-being.
Possessing the ability to change the way we think, is a gift in itself. Choosing to exercise our mental muscle builds resilience and resolve. Working on a brighter perspective won’t improve your eyesight, but it will help you see better.
Visual impairments range from minor to severe across a wide spectrum.Even the great majority of people meeting the qualification for “legal blindness” have significant usable sight. People generally exhibit an amazing ability to adjust and carry on. A positive outlook and can-do spirit are qualities key to success.
Here are a few steps toward a brighter perspective:
Acknowledge and value the vision you have. Take time each day to look around and appreciate the things you can see. Go for a walk in the park. Admire the ever-changing sky. Watch the sunrise or set.Get close up to see the face of someone you love and give them a kiss.
Live in the present, don’t waste precious time lamenting your vision past or future.
Give yourself credit for triumphs, even small ones. Every success builds confidence and buffers against depression.
Practice and repeat. The more you do, the better you get.
Use your experience to help others. Optimism is infectious.
Tell us: what keeps your glass half full?
This article was first published August 7, 2017 and refreshed August 20, 2020
Although life has slowed in some ways during the COVID pandemic, this is most likely not a time you are feeling at one with the universe.You may be experiencing a chronic sense of alarm, or a constant undercurrent of anxiety. And coping with vision loss, on top of that, usually adds its own layer of insecurity. Wouldn’t you love to find a way to get a daily dose of Zen?
Let’s try meditation. It doesn’t have to be difficult or time consuming for it to work, and you can begin benefitting from just a few minutes a day, right away. The more you do, the better you get. The simple act of being still and breathing deeply lowers stress hormones and can help with depression, anxiety and sleep issues. Meditation is a loving and mellow fitness program for your mind. No Sweat.
There are plenty of apps and guided meditations available to try, but the best way to begin a mediation practice may be this totally uncomplicated 4-step approach.
1. Designate a place to meditate each morning at the same time.
2. Mute your phone and turn off all other noise you can control.
3. Sit in a chair with back straight, shoulders relaxed, feet on the floor and hands in your lap with palms up or down. The idea is to be as neutral as possible so there’s no need to fidget.
4. Close your eyes and focus on your breathing. Take a long breath in and let it out slowly. Listen to the rhythm of your breathing.
Commit to at least 5 minutes each morning for the first week. When you feel ready, add a second meditation at the end of the day and increase the time of each practice to 10, 15 or 20 minutes as you progress.
To get started, keep it as simple as possible. Set a gentle timer so you won’t have to think about the time that has elapsed. Your mind will wander, that’s okay, bring it back to focus on the breathing. It may be helpful to count to 4 as you inhale and again as you exhale. Feel free to add some soothing music, a version of the lotus position, and a peaceful word or mantra, if you like.
This is simple, entry level meditating. Keep it up and feel the benefits, short term and long. Or let it be the springboard to becoming a Zen Master. Either way, it’s just minutes a day, and your mind, body and soul will thank you for it.
As ophthalmologists move from the urgent care-only phase, to scheduling routine eye exams again, it is important to know how patient safety is being protected. By now, all practices should be posting updated pandemic policies prominently on the homepage of their website, and including the update in the recorded messaging for patients contacting the office by phone. Being aware of the changes you will encounter during your next office visit will elevate your comfort and trust in the process.
Questions that need answers…
Can a telemedicine consultation be substituted for your in-person office visit.
How is staff being screened for COVID?
How is social distance being respected in waiting areas?
How is close contact being minimized in exam rooms between patients, doctors, technicians?
What is hand washing, sanitizing procedure?
What is frequency of sanitizing equipment and surfaces?
Are doctors and technicians wearing masks and using breath shields?
Patients should know they need to…
Cancel appointment if exposed to or symptomatic of COVID.
Be screened for COVID symptoms immediately before appointment.
Attend appointment alone, or get authorization for accompanying guest.
Wear a mask.
Wait to speak until exam is over and doctor or technician can move to a safe distance.
Send us your questions on this topic to [email protected]. We’ll be discussing it again in an upcoming OE Patients Podcast.
Image shows doctor consulting with patient on screen during video medical visit.
Urgent Care During Isolation
Social distancing measures are having a positive impact in slowing the spread of the coronavirus. They are also forcing change in the provision of healthcare. Ophthalmology, in particular, is conducted at close proximity, and it’s important to understand how that is being addressed. It is very likely that routine eye exams, check-ups and non-urgent procedures will be postponed for a few months. Communicate with your physician or contactthe office to clarify their specific and updated policies.
We consulted with our colleague, Yale L. Fisher, MD, retina specialist and founder of Ophthalmic Edge, to provide an overview of changes to patient care initiated by the COVID-19 crisis. To help you navigate the new normal, here are answers to frequently asked questions.
What is considered essential, urgent or emergent care?
Essential care is required, by the physician, to maintain or improve an ocular problem that is known. The physician should be contacted to determine if the treatment must be given on a specific regiment during this period.
Urgent and emergent care is marked by symptoms causing a sudden deterioration such as eye pain, a change in vision or visual field, double vision, blurred vision or swelling. Contact a doctor immediately for advice, or go to nearest eye hospital or medical center providing emergency services.
How does a patient decide when it’s appropriate to visit an ophthalmologist during social distancing restrictions?
There are many reasons requiring ongoing treatment or determinations of disease progression. A phone call and discussion with the physician is the best way to assess that need.
How have ophthalmic office procedures changed?
Most physicians have already altered their routine procedures to include COVID-19 guidelines, incorporating social distancing as well as masks, hand washing and rapid visits.
In what cases can video visits or telemedicine be substituted?
Video or telemedicine is useful especially for external eye examination. Questions and answers are definitely enhanced by video and audio communication. Some tests cannot be performed without imaging, especially for retinal or internal ocular problems. In some cases a local wide field photo and other tests can be performed and sent for evaluation by your physician.
How are patients, staff and doctors protected from spreading Coronavirus?
The same techniques as performed in medical facilities including social distance, masks worn by all, hand washing, sanitizing of surfaces, instruments and equipment.
Prioritizing your health means staying safe and strong during the COVID pandemic. It also means dealing appropriately with healthcare matters that should not be put off.As always, communication with your provider is is key.
This article was originally published April 17, 2020 and updated on June 5, 2020.
The COVID pandemic brought a sharp focus to the high risk category that combines factors of aging with underlying conditions. We asked OE contributor and wellness expert, Michelle Milgrim, to help us understand how we can stay healthy with age. Her advice is inspiring.
Research shows us that aging well is not just about what you eat.There are many modifiable lifestyle factors that contribute to the aging process in addition to eating, like exercise, sleep habits, building a social support system, and managing stress.Unfortunately, there are also some things we just can’t change that also play a part in how we age, like family health history and existing conditions.
Age is the single largest risk factor for heart disease and stroke, macular degeneration and cataracts, cancer, disability, and mental decline like Alzheimer’s, the sixth leading cause of death in United States.Living well into our older years is not simply about the absence of disease or conditions, but the quality of our days.Up to 30% of Medicare recipients report difficulties with routine activities of daily living, like eating, getting dressed, and taking a shower.
So what is within your power to not only live longer, but thrive in your later years?
The Nurses’ Health Study, one of the largest investigations into the risks of major chronic diseases, including eye disease, has informed many key findings about the aging process and practical tips for living well throughout our years.Most importantly, this study identified that 90% of chronic disease can be prevented by making a handful of key lifestyle changes.
Image shows youthful seniors exercising outdoors.
Maintain a healthy weight for your height, which means keeping your body mass index (BMI) within the normal range.For most, even a modest 5% weight loss can be enough to ease pressure on your lower joints making activity easier and more enjoyable, reduce risk of some cancers, prevent or delay type 2 diabetes, improve your lipid profile and reduce blood pressure, improve sleep, and reduce inflammation.
Make physical activity a regular habit.Finding something that you enjoy, are able to do most days of the week, and can participate in with others is key to creating a consistent exercise routine.Regular physical activity, in whatever form you enjoy, can not only support weight loss and reduce disease risk, but it can help you maintain cognitive function, sustain mobility, prevent falls, and provide an important outlet for building social connection.
Avoid tobacco.Quitting smoking is no easy task, but nicotine replacement therapies (NRT) have made it more approachable by reducing withdrawal symptoms and cigarette cravings.They have been found to double an individual’s chances of quitting for good.Tobacco cessation programs are a supportive complement to NRTs and are readily available in many communities, online or even via text on your mobile device. Visit SmokeFree.gov to learn more and get started.
Moderate alcohol intake.Research shows that the more alcohol a person drinks—particularly, the more alcohol consumed regularly over time—the greater the risk of developing specific cancers as well as other conditions like heart disease, stroke, and cognitive impairment.Drinking alcohol can also replace other fluids in our diet like water or calcium-rich milk, increasing the potential for dehydration and bone fracture as we get older.
Improve your diet.Follow a diet low in saturated fat, trans fat (mostly found in partially hydrogenated oils in processed foods) and sodium; limit intake of refined grains and sugary drinks; and eat more fruits, vegetables, legumes, nuts and unsaturated fats.This is the same basic healthy eating pattern that would benefit most regardless of age.
According to the Center for Disease Control and Prevention (CDC), only six percent of Americans engage in five key health-related behaviors that can prevent chronic disease, which includes getting enough sleep.About one-third of us manage to do at least three of these.So you’re in good company if you’re feeling overwhelmed by this idyllic list of goals.It’s not unattainable though.In fact, small changes can add up quickly and have a big impact on your personal well-being.If you’re not that active, consider adding a walk around the block after dinner with your spouse or a neighbor.If you’re diet leaves a bit to be desired, make one healthy swap at a single meal, like replacing half your usual morning bagel with an egg or low-fat Greek yogurt.If you’re drinking too much, cut back one drink at time, or alter your routine around the time you typically enjoy an adult beverage so you reduce the habitual craving.The idea is: think small then add small.Find small changes that you know you can make then up the ante each week or each month as the changes become an easier, more routine part of your lifestyle.
Image of fruits, veggies, legumes and nuts for healthy diet.
There are a few additional, unique dietary considerations as we reach the time of retirement:
Calories: Unfortunately, every year we get older, our resting metabolic rate declines, which simply means we need fewer calories to sustain our aging bodies.This can quickly lead to unwanted weight gain if we don’t make some adjustments to our diet or activity.Paying careful attention to what and how much you eat, as well as introducing resistance exercise to build or maintain muscle mass, are important to maintaining energy balance.Most healthy, older adults need between 1600 to 2400 calories per day depending on gender, age, and activity level.
Protein: Sarcopenia, or generalized loss of muscle mass and strength, can lead to frailty as we age.One way to combat this is to eat an adequate amount of high quality protein to support tissue maintenance and repair.The average adult needs between 45 to 60 grams protein daily.Higher quality protein sources include eggs, chicken, nonfat or low-fat milk, fish and lentils.
Vitamin B12:Our ability to absorb vitamin B12 naturally decreases as we age.The richest sources of B12 include meat, fish, poultry, eggs, and milk.If you’re still falling short or follow a vegan/vegetarian diet, you can speak with your doctor about a supplement.
Calcium and Vitamin D: Bone health becomes very important as we age.Making sure we get adequate calcium as well as vitamin D (to ensure the absorption of that calcium) is key to preventing osteoporosis and bone fractures.Dairy foods are the best source of dietary calcium because they are easily absorbed.Vitamin D is best found in fortified dairy products, but supplements can be used too.
Water:As we get older, our sensation for thirst actually decreases, which means we may reach for our water bottles less and less.Healthy adults need about 1.5 to 2 liters of fluid daily, including water, milk, and fruit juices.
It is possible to age like a fine wine,and like wine its better savored alongside a good meal in the company of friends.Keep physically and mentally active, invest in your interests, embrace the love and support of your family and friends, savor special foods in moderation and be mindful of eating a balanced plate at most meals, and try your best to get a good night’s rest.
Try this recipe for a delicious on-the-go snack or quick bite, try these Maple Roasted Chickpeas which are sure to please all the senses.
Maple Roasted Chickpeas
1 30 ounce can reduced sodium chickpeas, rinsed and drained
2 Tbsp. maple syrup
1 Tbsp. brown sugar
¼ tsp ground cayenne
¾ tsp cinnamon
½ tsp ground Ginger
Salt and black pepper to taste
Directions:Preheat oven to 425.Drain chickpeas and empty onto towel-lined baking sheet and pat until completely dry.Replace towel with parchment paper to line the baking sheet. Roast chickpeas in oven for 20 minutes, rotating and shaking halfway through cooking.Remove chickpeas and add to seasoning mixture.Coat chickpeas well and return to baking sheet.Bake another 10 to 15 minutes, or until crispy.
A visit to your eye doctor can come and go in a blur. Discussing a loss of sight is a dreadful thought — however, avoiding it will not yield positive results either. Time with the ophthalmologist may be brief, so it is important to be prepared and engaged. Considering these steps, before every appointment, will help you be an informed patient.
If you do not understand something the doctor says, or the terminology used, feel free to say, “I don’t understand, please explain.” Don’t be afraid to speak up.
Summarize back what you heard, to clarify your understanding. “So you are telling me that age-related macular degeneration will make me blind?” The doctor responds, “No, I am saying that there will be some loss of your central vision, possibly to the level of legal blindness, but macular degeneration does not cause total blindness.”
Request written materials, or even pictures or videos that you can take time to understand and absorb at home.
Ask about best-case and worst-case scenarios, and what is the most-likely scenario for you?
Image of ophthalmology office activity.
Write your questions and bring someone with you as an advocate, to read the questions on your behalf, and to take notes.
If treatment is available, understand the risks involved. “Can injections in the eye cause glaucoma?”
Ask if there is someone you can talk to, who is living with the condition, or has received the treatment.
If treatment is not available, ask for alternative therapies or lifestyle changes that may help your longterm prognosis and quality of life. Don’t accept “nothing can be done” for an answer.
If you are told nothing can be done to improve your vision, ask your ophthalmologist for information and resources to help you live successfully with vision loss, including referral to a low vision specialist and vision rehabilitation services.
It is crucial to be an Informed Patient when considering treatment or potential participation in a clinical trial. Clearly review, discuss and weigh the possible benefits against the risks. Consent forms are often many pages of medical and legal jargon — challenging for anyone to read, but especially hard with a visual impairment. Do not sign or agree to anything you have not read and understood completely.
January is Glaucoma Awareness Month, strategically placed at the start of each new year to remind us to schedule our annual comprehensive eye exam because early detection is still the best way to prevent the irreversible vision loss that can be caused quietly in the early stages and without noticeable symptoms. According to Prevent Blindness, more than 2.8 million Americans age 40 plus have glaucoma and nearly half do not know they have the disease.
When it comes to glaucoma awareness, it’s always a good time to improve your understanding and evaluate your risk.
Glaucoma is an increased pressure in the eyeball. It can be thought of as a “plumbing problem” with either too much fluid entering a closed system or not enough fluid going out. The result is an elevation in the intraocular pressure. Over time the pressure will irreversibly damage the optic nerve, which sends visual information from the retina to the brain.
There are no overt symptoms, so the vision loss which begins peripherally can quietly progress unnoticed. Early detection is key to saving sight. Regular comprehensive eye exams are the best way to detect glaucoma in its early stages. Although there is no cure, there is effective treatment. Eye drops are commonly prescribed to control the pressure.
You are at a higher risk for developing glaucoma if you have a family history (especially a sibling), are of African, Asian or Hispanic descent; are over age 60, have diabetes or are severely nearsighted. If you are affected by any other eye disease it is also important to have your pressure tested regularly.
Woman giving man eye pressure test. Credit: Mayo Clinic
It should also be noted that pressure problems often occur after retinal procedures and may last for short or long periods of time. Dependent on individual patient anatomy or pathology, these pressure changes require careful and sometimes immediate attention if permanent damage to the optic nerve is to be curtailed or prevented. Pressure elevations may even occur long after retinal procedures, a result of “altered” slow changes in tissues over time. While everyone should be aware of the need to check their intraocular pressure on a routine basis, those having undergone a retinal procedure should be especially vigilant in the immediate postoperative period and periodically thereafter. Often slow elevations occur without noticeable symptoms.
Should you find yourself in any of the risk categories mentioned, please consult your ophthalmologist and be meticulous in keeping up with your exams to avoid visual impairment, legal blindness, and potentially even total blindness.
Eyes with a dropper. Credit: RD.com
This article has been updated from original version published January 11, 2018.